




Ayushman Bharat Yojana Hospitals Empanelment Processes
1. Guidelines on Processes for Empanelment of Hospitals
1.1. Basic Principles
For providing the benefits envisaged under the Mission, the State Health Agency (SHA) through State Empanelment Committee (SEC) will empanel or cause to empanel private and public health care service providers and facilities in their respective State/UTs as per these guidelines.
The states are free to decide the mode of verification of empanelment application, conducting the physical verification either through District Empanelment Committee (DEC) or using the selected insurance company (Insurance Model), under the broad mandate of the instructions provided in these guidelines.
1.2. Institutional Set-Up for Empanelment
A. State Empanelment Committee (SEC) will constitute of following members:
CEO, State Health Agency – Chairperson;
Medical Officer not less than the level Director, preferably Director In Charge
for Implementation of Clinical Establishment Regulation Act – Member;
Two State government officials nominated by the Department – Members;
In case of Insurance Model, Insurance company to nominate a representative not below Additional General Manager or equivalent;
The state government may invite other members to SEC as it may deem fit to assist the
Committee in its activities. The State Government may also require the Insurance Company
to mandatorily provide a medical representative to assist the SEC in its activities.
Alternatively, the State/SHA may continue with any existing institution under the respective
state schemes that may be vested with the powers and responsibilities of SEC as per these
guidelines.
The SHAs through State Empanelment Committee (SEC) shall ensure:
Ensuring empanelment within the stipulated timeline for quick implementation
of the programme;
The empanelled provider meets the minimum criteria as defined by the
guidelines for general or specialty care facilities;
Empanelment and de-empanelment process transparency;
Time-bound processing of all applications; and
Time-bound escalation of appeals.
It is prescribed that at the district level, a similar committee, District Empanelment
Committee (DEC) will be formed which will be responsible for hospital empanelment related
activities at the district level and to assist the SEC in empanelment and disciplinary
proceedings with regards to network providers in their districts.
B. District Empanelment Committee (DEC) will constitute of the following members
Chief Medical Officer of the district
District Program Manager – State Health Agency
In case of Insurance Model, Insurance company representative
The State Government may require the Insurance Company to mandatorily provide a
medical representative to assist the DEC in its activities.
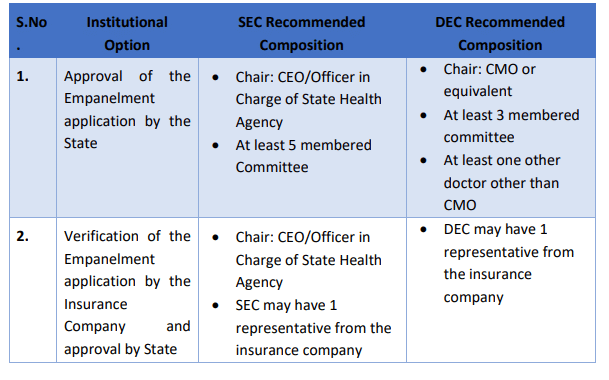
The structure of SEC and DEC for the two options are recommended as below:
The DEC will be responsible for:
Getting the field verification done along with the submission of the verification reports
to the SEC through the online empanelment portal.
The DEC will also be responsible for recommending, if applicable, any relaxation in
empanelment criteria that may be required to ensure that sufficient number of
empanelled facilities are available in the district.
Final approval of relaxation will lie with SEC
o The SEC will consider, among other things, the reports submitted by the DEC and
recommendation approve or deny or return to the hospital the empanelment
request.
1.3. Process of Empanelment
A. Empanelment requirements
i) All States/UTs will be permitted to empanel hospitals only in their own
State/UT.
ii) In case State/ UT wants to empanel hospitals in another State/UT, they can only
do so till the time that State/ UT is not implementing PMRSSM.
iii) All public facilities with capability of providing inpatient services (Community
Health Centre level and above) are deemed empanelled under PMRSSM. The
State Health Department shall ensure that the enabling infrastructure and
guidelines are put in place to enable all public health facilities to provide
services under PMRSSM.
iv) Employee State Insurance Corporation (ESIC) hospitals will also be eligible for
empanelment in PMRSSM, based on the approvals.
v) For private providers and not for profit hospitals, a tiered approach to
empanelment will be followed. Empanelment criteria are prepared for various
types of hospitals / specialties catered by the hospitals and attached in Annex 1.
vi) Private hospitals will be encouraged to provide ROHINI provided by Insurance
Information Bureau (IIB). Similarly public hospitals will be encouraged to have
NIN provided by MoHFW.
vii) Hospitals will be encouraged to attain quality milestones by making NABH pre
entry level accreditation mandatory for all the empaneled hospitals to be
attained within 1 year with 2 extensions of one year each.
viii)Hospitals with NABH accreditation will be given incentivised payment structures
by the states within the flexibility provided by MoHFW/NHA. The hospital with
NABH accreditation can be incentivized for higher package rates subject to
Procedure and Costing Guidelines.
ix) Hospitals in backwards/rural/naxal areas may be given incentivised payment
structures by the states within the flexibility provided by MoHFW/NHA
x) Criteria for empanelment has been divided into two broad categories as given
below
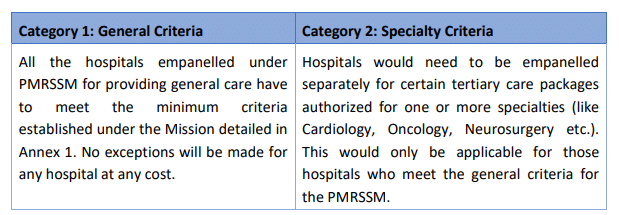
Detailed empanelment criteria have been provided as Annex 1.
State Governments will have the flexibility to revise/relax the empanelment criteria based,
barring minimum requirements of Quality as highlighted in Annex 1, on their local context,
availability of providers, and the need to balance quality and access; with prior approval
from National Health Agency. The same will have to be incorporated in the web-portal for
online empanelment of hospitals.
Hospitals will undergo a renewal process for empanelment once every 3 years or till the
expiry of validity of NABH certification whichever is earlier to determine compliance to
minimum standards.
National Health Agency may revise the empanelment criteria at any point during the
programme, if required and the states will have to undertake any required re-assessments
for the same.
1.4. Awareness Generation and Facilitation
The state government shall ensure that maximum number of eligible hospitals participate in
the PMRSSM, and this need to be achieved through IEC campaigns, collaboration with and
district, sub-district and block level workshops.
The state and district administration should strive to encourage all eligible hospitals in their
respective jurisdictions to apply for empanelment under PMRSSM. The SHA shall organise a
district workshop to discuss the details of the Mission (including empanelment criteria,
packages and processes) with the hospitals and address any query that they may have about
the mission.
Representatives of both public and private hospitals (both managerial and operational
persons) including officials from Insurance Company will be invited to participate in this
workshop
1.5. Online Empanelment
A. A web-based platform will be provided for empanelment of hospitals for PMRSSM.
B. The hospitals can apply through this portal only, as a first step for getting
empanelled in the programme.
C. This web-based platform will be the interface for application for empanelment of
hospitals under PMRSSM.
D. Following the workshop, the hospitals will be encouraged to initiate the process of empanelment through the web portal. Every hospital willing to get empanelled will need to visit the web portal, www.pmrssm.gov.in and create an account for themselve
E. Availability of PAN CARD number (not for public hospitals) and functional mobile number of the hospital will be mandatory for creation of this account / Login ID on the portal for the hospital.
F. Once the login ID is created, hospital shall apply for empanelment through an online application on the web portal – www.pmrssm.gov.in.
G. Each hospital will have to create a primary and a secondary user ID at the time of
registration. This will ensure that the application can be accessed from the
secondary user ID, in case the primary user is not available for some reason.
H. All the required information and documents will need to be uploaded and submitted by the hospital through the web portal.
I. Hospital will be mandated to apply for all specialties for which requisite infrastructure and facilities are available with it. Hospitals will not be permitted to choose specific specialties it wants to apply for unless it is a single specialty hospital.
J. After registering on the web-portal, the hospital user will be able to check the status of their application. At any point, the application shall fall into one of the following categories:
i) Hospital registered but application submission pending
ii) Application submitted but document verification pending
iii) Application submitted with documents verified and under scrutiny by DEC/SEC
iv) Application sent back to hospital for correction
v) Application sent for field inspection
vi) Inspection report submitted by DEC and decision pending at SEC level
vii) Application approved and contract pending
viii)Hospital empanelled
ix) Application rejected
x) Hospital de-empanelled
xi) Hospital blacklisted (2 years)
1.6. Role of DEC
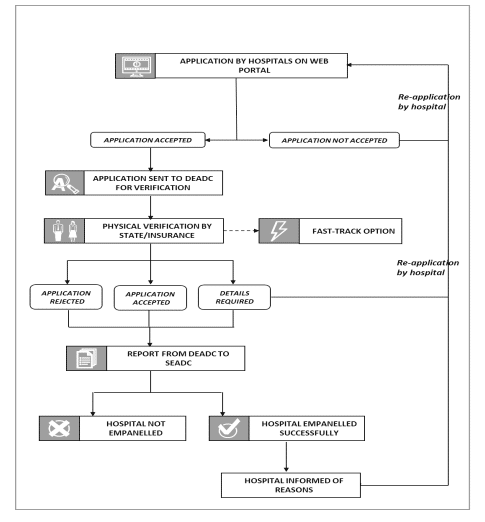
A. After the empanelment request by a hospital is filed, the application should be scrutinized by the DEC and processed completely within 15 days of receipt of application.
B. A login account for a nodal officer from DEC will be created by SEC. This login ID will
be used to download the application of hospitals and upload the inspection report.
C. As a first step, the documents uploaded have to be correlated with physical – verification of original documents produced by the hospital. In case any documents are found wanting, the DEC may return the application to the hospital for rectifying any errors in the documents.
D. After the verification of documents, the DEC will physically inspect the premises of
the hospital and verify the physical presence of the details entered in the empanelment application, including but not limited to equipment, human resources, service standards and quality and submit a report in a said format through the portal along with supporting pictures/videos/document scans
E. DEC will ensure the visits are conducted for the physical verification of the hospital. The verification team will have at least one qualified medical doctor (minimum MBBS).
F. The team will verify the information provided by the hospitals on the web-portal and will also verify that hospitals have applied for empanelment for all specialties as available in the hospital.
G. In case during inspection, it is found that hospital has not applied for one or more specialties but the same facilities are available, then the hospital will be instructed to apply for the missing specialties within a stipulated a timeline (i.e. 7 days from the inspection date).
i) In this case, the hospital will need to fill the application form again on the web portal. However, all the previously filled information by the hospital will be prepopulated and hospital will be expected to enter the new information.
ii) If the hospital does not apply for the other specialties in the stipulated time, it will be disqualified from the empanelment process.
H. In case during inspection, it is found that hospital has applied for multiple
specialties, but all do not conform to minimum requirements under PMRSSM then
the hospital will only be empanelled for specialties that conform to PMRSSM norms.
I. The team will recommend whether hospital should be empanelled or not based on
their field-based inspection/verification report.
J. DEC team will submit its final inspection report to the state. The district nodal officer
has to upload the reports through the portal login assigned to him/her.
K. The DEC will then forward the application along with its recommendation to the SEC.
1.7. Role of SEC
A. The SEC will consider, among other things, the reports submitted by the DEC and
recommendation approve or deny or return back to the hospital the empanelment
request.
B. In case of refusal, the SEC will record in writing the reasons for refusal and either
direct the hospital to remedy the deficiencies, or in case of egregious emissions from
the empanelment request, either based on documentary or physical verification,
direct the hospital to submit a fresh request for empanelment on the online portal.
C. The SEC will also consider recommendations for relaxation of criteria of
empanelment received from DEC or from the SHA and approve them to ensure that
sufficient number and specialties of empanelled facilities are available in the states.
D. Hospital will be intimated as soon as a decision is taken regarding its empanelment
and the same will be updated on the PMRSSM web portal. The hospital will also be
notified through SMS/email of the final decision. If the application is approved, the
hospital will be assigned a unique national hospital registration number under
PMRSSM.
E. If the application is rejected, the hospital will be intimated of the reasons on the
basis of which the application was not accepted and comments supporting the
decision will be provided on the PMRSSM web portal. Such hospitals shall have the
right to file a review against the rejection with the State Health Agency within 15
days of rejection through the portal. In case the request for empanelment is rejected
by the SHA in review, the hospitals can approach the Grievance Redressal
Mechanism for remedy.
F. In case the hospital chooses to withdraw from PMRSSM, it will only be permitted to
re-enter/ get re-empanelled under PMRSSM after a period of 6 months.
G. If a hospital is blacklisted for a defined period due to fraud/abuse, after following due process by the State Empanelment Committee, it can be permitted to re-apply after cessation of the blacklisting period or revocation of the blacklisting order, whichever is earlier.
H. There shall be no restriction on the number of hospitals that can be empanelled
under PMRSSM in a district.
I. Final decision on request of a Hospital for empanelment under PMRSSM, shall be
completed within 30 days of receiving such an application.
1.8. Fast Track Approvals
A. In order to fast track the empanelment process, hospitals which are NABH accredited
shall be auto-empaneled provided they have submitted the application on web portal
and meet the minimum criteria.
B. In order to fast track the empanelment process, the states may choose to autoapprove
the already empanelled hospitals under an active RSBY scheme or any other
state scheme; provided that they meet the minimum eligibility criteria prescribed
under PMRSSM.
C. If already empanelled, under this route, should the state allow the auto-approval
mode, the hospital should submit their RSBY government empanelment ID or State
empanelment ID during the application process on the web portal to facilitate onboarding
of such service providers.
D. The SEC shall ensure that all hospitals provided empanelment under Fast Track
Approval shall undergo the physical verification process within 3 months of approval. If
a hospital is found to have wrongfully empanelled under PMRSSM under any category,
such an empanelment shall be revoked to the extent necessary and disciplinary action
shall be taken against such an errant medical facility.
1.9. Signing of Contract
A. Within 7 days of approval of empanelment request by SEC, the State Government will
sign a contract with the empanelled hospitals as per the template defined in the tender
document.
B. If insurance company is involved in implementing the scheme in the State, they will also
be part of this agreement, i.e. tripartite agreement will be made between the IC, SHA
and the hospital.
C. Each empanelled hospital will need to provide a name of a nodal officers who will be the focal point for the PMRSSM for administrative and medical purposes.
D. Once the hospital is empanelled, a separate admin user for the hospital will be created
to carry out transactions for providing treatment to the beneficiaries.
1.10. Process for Disciplinary Proceedings and De-Empanelment
A. Institutional Mechanism
i) De-empanelment process can be initiated by Insurance Company/SHA after
conducting proper disciplinary proceedings against empanelled hospitals on
misrepresentation of claims, fraudulent billing, wrongful beneficiary
identification, overcharging, unnecessary procedures, false/misdiagnosis,
referral misuse and other frauds that impact delivery of care to eligible
beneficiaries.
ii) Hospital can contest the action of de-empanelment by Insurance Company with SEC/SHA. If hospital is aggrieved with actions of SEC/SHA, the former can approach the SHA to review its decision, following which it can request for redressal through the Grievance Redressal Mechanism as per guidelines.
iii) In case of implementation through the insurance mode, the SEC and DEC will mandatorily include a representative of the Insurance Company when deliberating and deciding on disciplinary proceedings under the scheme.
iv) The SEC may also initiate disciplinary proceedings based on field audit
reports/survey reports/feedback reports/ complaints filed with them/
complaints.
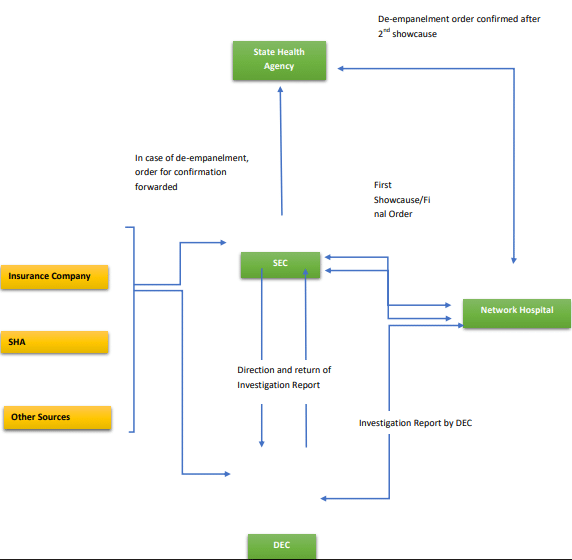
v) For disciplinary proceedings, the DEC may consider submissions made by the beneficiaries (through call centre/written submissions/Emails etc.) or directions from SEC or information from other sources to investigate a claim of fraud by a hospital.
vi) On taking up such a case for fraud, after following the procedure defined, the DEC will forward its report to the SEC along with its recommendation for action to be taken based on the investigation.
vii) The SEC will consider all such reports from the DECs and pass an order detailing the case and the penalty provisions levied on the hospital.
viii) Any disciplinary proceeding so initiated shall have to be completed within 30
days.
B. Steps for Disciplinary Proceedings
Step 1 – Putting the provider on “Watch-list”
Based on the claims, data analysis and/or the provider visits, if there is any doubt on the performance of a Provider, the SEC on the request of the IC or the SHA or on its own findings or on the findings of the DEC, can put that hospital on the watch list. The data of such hospital shall be analysed very closely on a daily basis by the SHA/SEC for patterns, trends and anomalies and flagged events/patterns will be brought to the scrutiny of the DEC and the SEC as the case may be.
The IC shall notify such service provider that it has been put on the watch-list and
the reasons for the same.
Step 2 – Issuing show-cause notice to the hospital
Based on the activities of the hospital if the insurer/ trust believes that there are clear grounds of hospital indulging in wrong practices, a showcause notice shall be issued to the hospital. Hospital will need to respond to the notice within 7 days of receiving it.
Step 3 – Suspension of the hospital
A Provider can be temporarily suspended in the following cases:
i) For the Providers which are on the “Watch-list” or have been issued showcause notice if the SEC observes continuous patterns or strong evidence of irregularity based on either claims data or field visit of the hospital or in case of unsatisfactory reply of the hospital to the showcause notice, the
hospital may be suspended from providing services to beneficiaries under the scheme and a formal investigation shall be instituted.
ii) If a Provider is not in the “Watch-list”, but the SEC observes at any stage that it has data/ evidence that suggests that the Provider is involved in any unethical Practice/ is not adhering to the major clauses of the contract with the Insurance Company / Involved in financial fraud related to health insurance patients, it may immediately suspend the Provider from providing services to policyholders/insured patients and a formal investigation shall be instituted.
A formal letter shall be send to the concerned hospital regarding its suspension with
mentioning the time frame within which the formal investigation will be completed.
Step 4 – Detailed Investigation
The detailed investigation shall be undertaken for verification of issues raised in
disciplinary proceedings and may include field visits to the providers, examination of
case papers, talking with the beneficiary/ policyholders/insured (if needed), examination of provider records etc. If the investigation reveals that the report/
complaint/ allegation against the provider is not substantiated, the Insurance
Company/SHA would immediately revoke the suspension (in case of suspension) on
the direction of the SEC. A letter regarding revocation of suspension shall be sent to
the provider within 24 hours of that decision.
Step 5 – Presentation of Evidence to the SEC
The detailed investigation report should be presented to the SEC and the detailed
investigation should be carried out in stipulated time period of not more than 7 days.
The insurance company (Insurance mode)/SHA (Trust Mode) will present the findings
of the detailed investigation. If the investigation reveals that the
complaint/allegation against the provider is correct, then the following procedure
shall be followed:
i) The hospital must be issued a “show-cause” notice seeking an explanation
for the aberration.
ii) In case the proceedings are under the SEC, after receipt of the explanation
and its examination, the charges may be dropped or modified or an action
can be taken as per the guidelines depending on the severity of the
malafide/error. In cases of de-empanelment, a second show cause shall be
issued to the hospital to make a representation against the order and after
considering the reply to the second showcause, the SEC can pass a final order
on de-empanelment. If the hospital is aggrieved with actions of SEC/SHA, the
former can approach the SHA to review its decision, following which it can
request for redressal through the Grievance Redressal Mechanism as per
guidelines.
iii) In case the preliminary proceedings are under the DEC, the DEC will have to
forward the report to the SEC along with its findings and recommendations
for a final decision. The SEC may ask for any additional
material/investigation to be brought on record and to consider all the
material at hand before issuing a final order for the same.
The entire process should be completed within 30 days from the date of suspension.
The disciplinary proceedings shall also be undertaken through the online portal only.
Step 6 – Actions to be taken after De- empanelment
Once the hospital has been de-empanelled, following steps shall be taken:
i) A letter shall be sent to the hospital regarding this decision.
ii) A decision may be taken by the SEC to ask the SHA/Insurance Company to
lodge an FIR in case there is suspicion of criminal activity
iii) This information shall be sent to all the other Insurance Companies as well as
other regulatory bodies and the MoHFW/ NHA.
iv) The SHA may be advised to notify the same in the local media, informing all
policyholders/insured about the de-empanelment ensuring that the
beneficiaries are aware that the said hospital will not be providing services
under PMRSSM.
v) A de-empanelled hospital cannot re-apply for empanelment for at least 2
years after de-empanelment. However, if the order for de-empanelment
mentions a longer period, such a period shall apply for such a hospital.
C. Gradation of Offences
On the basis of the investigation report/field audits, the following charges may be found to
be reasonably proved and a gradation of penalties may be levied by the SEC. However, this
tabulation is intended to be as guidelines rather than mandatory rules and the SEC may take
a final call on the severity and quantum of punishment on a case to case basis.
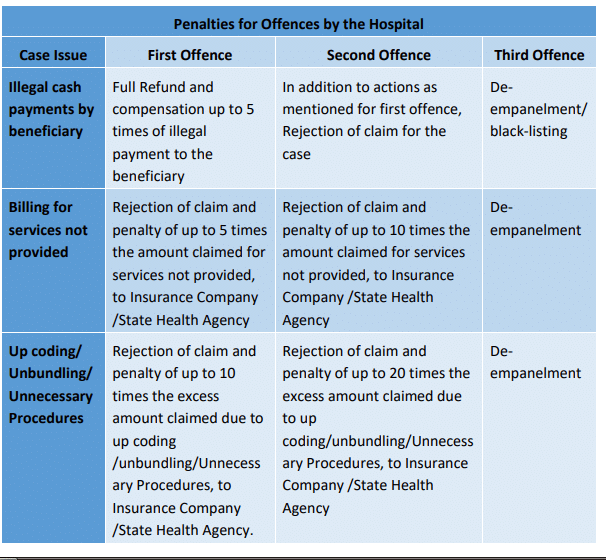
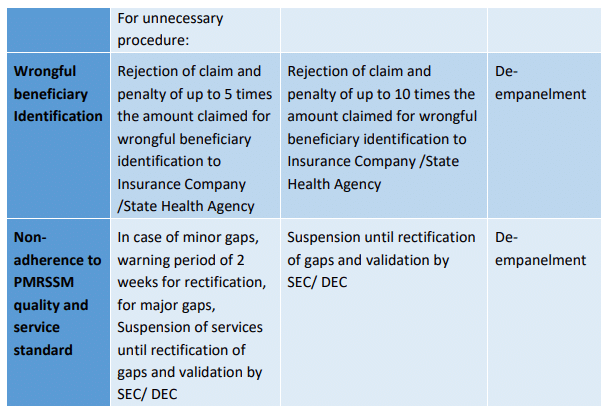
All these penalties are recommendatory and the SEC may inflict larger or smaller penalties
depending on the severity/regularity/scale/intentionality on a case to case basis with
reasons mentioned clearly in a speaking order
Annex 1: Detailed Empanelment Criteria
Minimum Criteria
A Hospital would be empanelled as a network private hospital with the approval of the
respective State Health Authority1
if it adheres with the following minimum criteria:
1. Should have at least 10 inpatient beds with adequate spacing and supporting staff as
per norms.
i. Exemption may be given for single-specialty hospitals and in remote/ rural areas (as currently practiced under RSBY).
ii. In case of providing surgical packages a minimum of 15 beds is prescribed.
2. It should have adequate and qualified medical and nursing staff (doctors2 & nurses3
), physically in charge round the clock; (necessary certificates to be produced during
empanelment).
3. Fully equipped and engaged in providing Medical and Surgical services,
commensurate to the scope of service/ available specialities and number of beds.
i. Round-the-clock availability (or on-call) of a Surgeon and Anaesthetist where
surgical services/ day care treatments are offered.
ii. Round-the-clock availability (or on-call) of an Obstetrician, Paediatrician and
Anaesthetist where maternity services are offered.
iii. Round-the-clock availability of specialists (or on-call) in the concerned
specialties having sufficient experience where such services are offered (e.g.
Orthopaedics, ENT, Ophthalmology, Dental, general surgery (including
endoscopy) etc.)
4. Hospital should have adequate arrangements for round-the-clock support systems
required for the above services like Pharmacy, Blood Bank, Laboratory, Dialysis unit,
Endoscopy investigation support, Post op ICU care with ventilator support
(mandatory for providing surgical packages), X-ray facility etc., either ‘In-House’ or
with ‘Outsourcing arrangements’ with appropriate agreements and in nearby
vicinity.
5. Round-the-clock Ambulance facilities (own or tie-up).
6. 24 hours emergency services managed by technically qualified staff wherever
emergency services are offered
7. Casualty should be equipped with Monitors, Defibrillator, Nebulizer with accessories,
Crash Cart, Resuscitation equipment, Oxygen cylinders with flow meter/
tubing/catheter/face mask/nasal prongs, Suction apparatus etc. and with attached
toilet facility. Mandatory for hospitals wherever surgical procedures are offered:
i. Fully equipped Operation Theatre of its own with qualified nursing staff
under its employment round the clock.
ii. Post-op ward with ventilator and other required facilities.
8. Wherever intensive care services are offered it is mandatory to be equipped with an
Intensive Care Unit (For medical/surgical ICU/HDU) with requisite staff
i. The unit is to be situated in close proximity of operation theatre, acute care
medical and surgical ward units.
ii. Suction, oxygen supply and compressed air should be provided for each bed.
iii. Further High Dependency Unit (HDU) – where such packages are mandated
should have the following equipment:
1) Piped gases
2) Multi-sign Monitoring equipment
3) Infusion of ionotropic support
4) Equipment for maintenance of body temperature
5) Weighing scale
6) Manpower for 24×7 monitoring
iv. ICU should also be equipped with all the equipment and manpower as per
HDU norms, plus paediatric ventilator(s).
9. Records Maintenance: Maintain complete records as required on day-to-day basis
and is able to provide necessary records of hospital / patients to the Society/Insurer
or his representative as and when required.
i. Wherever automated systems are used it should comply with MoHFW/ NHA
EHR guidelines (as and when they are enforced and updated)
ii. All PMRSSM cases must have complete records maintained
10. Legal requirements as applicable by the local/state health authority.
11. Adherence to Standard treatment guidelines/ Clinical Pathways for procedures as
mandated by NHA from time to time.
12. Registration with the Income Tax Department.
13. NEFT enabled bank account
14. Telephone/Fax
15. Safe drinking water facilities.
16. Uninterrupted (24 hour) supply of electricity and generator facility with required
capacity suitable to the bed strength of the hospital.
17. Waste management support services (General and Bio Medical) – in compliance with
the bio-medical waste management act.
18. Appropriate fire-safety measures.
19. Provide space for a separate kiosk for PMRSSM beneficiary management (PMRSSM
non-medical4
coordinator) at the hospital reception.
20. Ensure a dedicated medical officer to work as a medical5
co-ordinator towards
PMRSSM beneficiary management (including records for follow-up care as
prescribed)
21. Ensure appropriate promotion of PMRSSM in and around the hospital (display
banners, brochures etc.) towards effective publicity of the scheme in co-ordination
with the SHA/ district level PMRSSM team.
22. IT Hardware requirements (desktop/laptop with internet, printer, webcam, scanner/
fax, bio-metric device etc.) as mandated by the NHA
Advanced Criteria
Over and above the essential criteria required to provide basic services under PMRSSM (as
mentioned in Category 1) those facilities undertaking defined speciality packages (as
indicated in the benefit package for specialities mandated to qualify for advanced criteria)
should have the following:
1. These empanelled hospitals may provide specialized services such as Cardiology,
Cardiothoracic surgery, Neurosurgery, Nephrology, Reconstructive surgery,
Oncology, Neonatal/ Paediatric Surgery, Urology etc.
2. A hospital could be empanelled for one or more specialities subject to it qualifying to
the concerned speciality criteria.
3. Such hospitals should be fully equipped with ICCU/SICU/ NICU/ relevant Intensive
Care Unit in addition to and in support of the OT facilities that they have.
4. Such facilities should be of adequate capacity and numbers so that they can handle
all the patients operated in emergencies.
i. The Hospital should have sufficient experienced specialists with an advanced
qualification in the specific identified fields for which the Hospital is
empanelled as per the requirements of professional and regulatory bodies/
as specified in the clinical establishment act/ State regulations.
(4 . The non-medical coordinator will do a concierge and helpdesk role for the patients visiting the hospital, acting as a facilitator for beneficiaries and are the face of interaction for the beneficiaries. Their role will include helping in preauthorization, claim settlement,
follow-up and Kiosk-management (including proper communication of the scheme).
5. The medical coordinator will be an identified doctor in the hospital who will facilitate submission of online pre-authorization and claims requests, follow up for meeting any deficiencies and coordinating necessary and appropriate treatment in the hospital.)
ii. The Hospital should have sufficient diagnostic equipment and support
services in the specific identified fields for which the Hospital is empanelled
as per the requirements specified in the clinical establishment act/ State
regulations as the case may be.
5. Indicative speciality specific criteria are as under:
Specific Criteria for Cardiology/ CVTS
1. CTVS theatre facility (Open Heart Tray, Gas pipelines Lung Machine with TCM,
defibrillator, ABG Machine, ACT Machine, Hypothermia machine, IABP, cautery etc.)
2. Post-op with ventilator support
3. ICU Facility with cardiac monitoring and ventilator support
4. Hospital should facilitate round the clock cardiologist services.
5. Availability of support speciality of General Physician & Paediatrician
6. Fully equipped Catheterization Laboratory Unit with qualified and trained
Paramedics.
Specific Criteria for Cancer Care
1. The facility should have a tumour board which decides a comprehensive plan
towards multi-modal treatment of the patient or if not, then appropriate linkage
mechanisms need to be established to the nearest regional cancer centre (RCC).
Tumour board should consist of a qualified team of Surgical, Radiation and Medical
Oncologist in order to ensure the most appropriate treatment for the patient.
2. Relapse/recurrence may sometimes occur during/ after treatment. Retreatment is
often possible which may be undertaken after evaluation by a Medical/ Paediatric
Oncologist/ tumor board with prior approval and pre-authorization of treatment.
3. For extending the treatment of chemotherapy and radiotherapy the hospital should
have the requisite infrastructure for radiotherapy treatment viz. for cobalt therapy,
linear accelerator radiation treatment and brachytherapy available in-house or
through “outsourced facility”. In case of outsourced facility, the empanelled hospital
for radiotherapy treatment and even for chemotherapy, shall not perform the
approved surgical procedure alone, but refer the patients to other centres for followup
treatments requiring chemotherapy and radiotherapy treatments. This should be
indicated where appropriate in the treatment approval plan.
4. Further hospitals should have infrastructure capable for providing certain specialized
radiation treatment packages such as stereotactic radiosurgery/ therapy.
i. Treatment machines which are capable of delivering SRS/SRT
ii. Associated Treatment planning system
iii. Associated Dosimetry systems
Specific Criteria for Neurosurgery
1. Well Equipped Theatre with qualified paramedical staff, C-Arm, Microscope,
neurosurgery compatible OT table with head holding frame (horseshoe, may
field/sagittal or equivalent frame).
2. Neuro ICU facility
3. Post-op with ventilator support
4. Facilitation for round the clock MRI, CT and other support bio-chemical
investigations.
Specific Criteria for Burns, Plastic & Reconstructive surgery
1. The Hospital should have full time/on-call services of qualified plastic surgeon and
support staff with requisite infrastructure for corrective surgeries for post burn
contractures.
2. Isolation ward having monitor, defibrillator, central oxygen line and all OT
equipment.
3. Well Equipped Theatre
4. Surgical Intensive Care Unit.
5. Post-op with ventilator support
6. Trained Paramedics
7. Post-op rehab/ Physiotherapy support/ Phycology support.
Specific Criteria for Neonatal/Paediatric Surgery
1. The Hospital should have full time/on call services of paediatric surgeons / plastic
surgeons / urologist surgeons related to congenital malformation in the paediatric
age group.
2. Well-equipped theatre
3. Paediatric and Neonatal ICU support
4. NICU should be divided into 2 portions, one for clean babies and other for septic
babies.
5. NICU should be Equipped with Ventilators, Phototherapy Units, Transport
incubators, Nebulizer, Pulse oxymeter, Multi-para monitors, Syringe pumps, Infusion
pumps, Resuscitation trolley.
6. Support services of paediatrician (should be in-charge of NICU).
7. Availability of mother rooms and feeding area.
8. Availability of radiological/ fluoroscopy services (including IITV), Laboratory services
and Blood bank either “inhouse” or through outsourced facility.
Specific Criteria for Polytrauma
1. Shall have Emergency Room Setup with round the clock dedicated duty doctors.
2. Shall have the full-time service availability of Orthopaedic Surgeon, General Surgeon,
and anaesthetist services.
3. The Hospital shall provide round the clock services of Neurosurgeon, Orthopaedic
Surgeon, CT Surgeon, General Surgeon, Vascular Surgeon and other support
specialists as and when required based on the need.
4. Shall have dedicated round the clock Emergency theatre with C-Arm facility, Surgical
ICU, Post-Op Setup with qualified staff.
5. Shall be able to provide necessary diagnostic support round the clock including
specialized investigations such as CT, MRI, emergency biochemical investigations.
Specific criteria for Nephrology and Urology Surgery
1. Dialysis unit
2. Well-equipped operation theatre with C-ARM
3. Endoscopy investigation support
4. Post op ICU care with ventilator support
5. Sew lithotripsy equipment either “in-house” or through outsourced facility
Annex 2: Process Flow for the Empanelment
Related Post on Ayushman Bharat | PM – Jan Arogya Yojana
Free Study Material on PM – Jan Arogya Yojana
Check Am I Eligible for Ayushman Bharat | PM – Jan Arogya Yojana
Ayushman Bharat : Policy & Guidelines : PM-JAY
Ayushman Mitra : Guidelines under PM-JAY
Ayushman Bharat : Annexure-1 PreAuthorization Form :Download /Print
Ayushman Bharat : Annexure II – Discharge Summary : Download /Print
Website mera.pmjay.gov.in for Ayushman Bharat
Ayushman Bharat launched by PM on 23.09.2018; PMJAY at Ranchi
Ayushman Bharat Yojana :Pradhan Mantri Jan Aarogya Yojana Features :
Use of Aadhaar in Ayushman Bharat – Desirable and not “Must”
Ayushman Bharat – National Health Protection Mission : Features